Bread and Prejudice: Redesigning Digital Food Environments for Health Equity
This project proposes a kiosk interface redesign for UK takeaway chains to reduce calorie intake in the most deprived communities by changing the digital food environment rather than people’s willpower. It combines behavioural science, public health policy, and service design to align a kiosk-based intervention with the Department of Health and Social Care (DHSC) and the National Health Service (NHS) prevention priorities.
Role: Behavioural intervention · Service design
The Problem
Fast-food outlets are more concentrated in deprived areas than in affluent ones, with this gap widening by 28% between 2011 and 2024, without a corresponding expansion in supermarkets offering healthier choices. In these same communities, food choices are shaped more by immediate environment and convenience than by health knowledge, which limits the impact of awareness-driven interventions.
At the same time, self-service kiosks have become a major access point for takeaway food, with around 58% of UK food outlets adopting kiosk technology since 2020, a share that continues to grow. Industry guidance encourages operators to prioritise profitable items on opening screens, use enticing visuals, and embed upsell prompts that increase calories per transaction, creating digital “dark patterns” that push users toward high-calorie choices without their conscious awareness.
Goals
-
Target the structural, environmental determinants of unhealthy eating in deprived communities, rather than individual motivation or knowledge.
-
Redesign the digital food ordering moment (self-service kiosks) to make healthier options more salient, accessible, and default, without removing choice or increasing cognitive burden.
-
Develop a DHSC-ready intervention that fits within existing regulatory and NHS strategic frameworks, is operationally feasible at scale, and can be piloted and evaluated through existing transaction data.
Users and Stakeholders
-
Primary users:
-
Time-pressed consumers in deprived UK areas using self-service kiosks, especially families and low-income individuals whose choices are driven by System 1 processes.
-
-
Institutional stakeholders:
-
Department of Health and Social Care (DHSC), as the primary policy audience and implementation sponsor
-
-
Commercial stakeholders:
-
Quick-service restaurant operators (e.g., kiosk-based chains) who control kiosk configuration and may be concerned about revenue impacts
-
-
Implementation ecosystem:
-
Kiosk vendors and software providers responsible for interface design and configuration
-
Local authorities in high-deprivation, high-takeaway regions where pilots would be prioritised
-
Empirical Evidence
The intervention is grounded in a review of policy evaluations, behavioural science, and service design literature.
-
Evaluations of the Soft Drinks Industry Levy, which show significant reductions in sugar content and greater health gains among deprived communities, demonstrate that structural product changes can reduce inequalities.
-
Studies on menu positioning and defaults show that placing healthier items higher on menus and setting them as defaults increases selection rates, particularly among low-income or low-literacy groups.
-
Systematic reviews indicate that colour-coded labels and contextual calorie references at the point of purchase (rather than on packaging alone) can shift choices toward lower-calorie options.
-
Experimental work demonstrating that digital menu reordering (e.g., in delivery apps) can nudge users across socioeconomic groups toward lower-calorie meals.
Constraints
-
Policy design constraints:
-
The intervention must operate within existing out-of-home food regulations and avoid the need for primary legislation, mirroring how calorie labelling was implemented.
-
-
Scope constraints:
-
The intervention focuses on three TIPPME dimensions: Position, Functionality, and Presentation, because other dimensions like size, availability, and proximity require physical or supply-chain changes beyond kiosk configuration.
-
-
Operational constraints:
-
Implementation depends on vendor compliance, staff training, and consistent digital monitoring, with risks around delayed software updates, neglected defaults, and logistical practices that could reintroduce unhealthy biases
-
Collectively, these changes are designed to shift the “path of least resistance” toward lower-calorie choices without restricting options or increasing cognitive load.
Solution
A. Position – Restructuring the opening screen
-
Opening screen shows only meals at or below 600 kcal (NHS guideline), ordered in ascending calories.
-
Full menu remains one tap away; no items are removed, only reordered.
Design principle
Make healthier options the easiest to see and select, using positioning rather than persuasion.
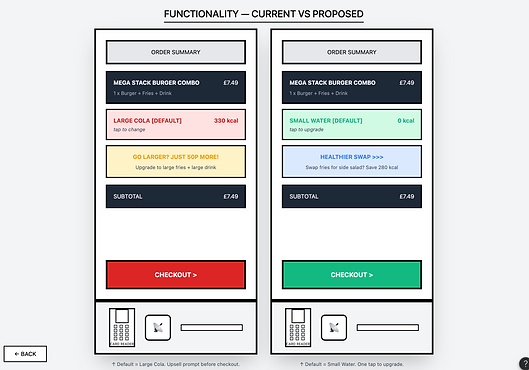
B. Functionality – Defaults and “Healthier Swap”
-
Default drink is preset to the smallest size or a low-sugar option, with a visible upgrade choice.
-
A one-tap “Healthier Swap” prompt appears on the order summary screen before checkout, offering a quick switch to a healthier equivalent.
Design principle
Use defaults and a brief “reflection window” to shift the path of least resistance without adding friction.
C. Presentation – Colour-coded cues
-
Each item carries a traffic light colour-coded calorie dot, plus a standard note: adults need around 2000 kcal a day.
-
Labels appear on the transaction screen in real time, recognising that raw calorie numbers are hard to interpret for time-pressed, lower-income consumers.
Design principle
Make calorie information instantly interpretable using simple visual cues instead of dense text.
Design Process
The design process is evidence-led and policy-focused rather than a conventional UX sprint.
-
Policy gap mapping
-
Analyse how existing UK interventions (e.g., SDIL, ad bans, calorie labelling) miss the digital ordering moment.
-
-
Environment diagnosis
-
Examine kiosk flows as “dark pattern” environments designed to maximise calories per transaction through default prompts, item order, and visuals.
-
-
Framework selection
-
Adopt the TIPPME typology to structure environmental interventions that can be centrally configured and deployed across locations.
-
-
Intervention design
-
Translate evidence on defaults, menu order, and colour coding into specific kiosk changes for Position, Functionality, and Presentation.
-
-
Implementation blueprinting
-
Align with NHS and DHSC tools, using kiosk transaction data to evaluate changes over time.
-
Evidence for effectiveness
The intervention targets fast, automatic (System 1) decisions in timed kiosk flows, where people usually accept the first or default option rather than investing effort to switch. Studies show that nudges and defaults have the strongest effects for low-income groups with lower knowledge and literacy, and that reordering digital menus can shift choices toward lower-calorie items across socioeconomic groups. Field evidence from UK cafeterias suggests that healthier defaults can change choices without reducing revenue, addressing likely operator concerns.
Public acceptability
For a parent in Sunderland, prices and items stay the same; what changes is what appears first, what is preselected, and the presence of simple colour-coded calorie cues, with one tap to see the full menu. People tend to support interventions that reshape how options are presented instead of banning items, and this is particularly relevant in deprived areas with the worst diets and highest free sugar intake. Using existing food service regulations, kiosk configuration standards can be introduced first in high-deprivation areas, with transaction data used to track calorie purchases across phased pilots before any wider scaling.
Implementation Plan
Regulatory path
-
Introduce kiosk configuration standards, similar to calorie labelling guidance, through existing out-of-home sector regulations.
-
Embed within NHS England’s 10-year health plan as a prevention-focused digital environment change.
Phased rollout
-
Phase 1: Pilot in the most deprived, high-takeaway areas, using existing kiosk transaction logs to track calorie purchases before and after.
-
Phase 2: Extend to deprived urban regions with high kiosk penetration.
-
Phase 3: Scale nationwide, contingent on evidence from earlier phases.
Service blueprint highlights
-
Standard configurations across vendors.
-
Training and monitoring to keep defaults and menu order intact over time.
Projected Impact
Behavioural
-
Expected reduction in average calories per transaction by making healthier options more salient, preselected, and easier to interpret at the point of purchase, especially under time pressure.
Equity
-
Because defaults and nudges often have stronger effects among low-income and low-literacy groups, the intervention is designed to benefit those whom awareness campaigns have failed to reach.
Economic
-
Evidence from similar cafeteria interventions suggests that healthier defaults do not inherently reduce revenue, giving a partial basis for operator reassurance.
Risks and Trade-offs
-
Effect size risk: Evidence comes mainly from controlled environments; real-world effects may be smaller.
-
Operational risk: Vendor resistance, delayed updates, and “workarounds” could erode the integrity of defaults and menu ordering.
-
Ethical trade-off: Interventions deliberately steer behaviour via choice architecture, though they avoid bans and maintain full menu availability, aligning with public preferences for showcasing rather than removing options.
These are treated as implementation watchouts, not reasons to discard the idea.